
Prescription for Ontario
Doctors aim to make the system better for all of us
Prescription for Ontario: Doctors’ 5-Point Plan for Better Health Care, released in October 2021, outlines the actions necessary to fix the province’s health-care system. It provides 87 recommendations to address new and long-standing issues in the overall system, including 12 that speak to the unique barriers to adequate health care in northern Ontario.
The Prescription for Ontario was informed by the largest consultation in its 140-year history. More than 1,600 physicians and physician leaders provided their expert advice. More than 110 health-care stakeholders, social service agencies and community leaders offered solutions from their unique perspectives. Almost 8,000 Ontarians, representing 600 communities, shared their health-care priorities through an online survey.
A second round of consultations with members and stakeholders resulted in the OMA's development of a progress report in May 2023 designed to measure the successes and failures to date in implementing the original recommendations and help guide its advocacy efforts going forward.
Since then, the OMA consulted broadly and brought together the collective expertise of physicians and other key stakeholders to find tangible and immediate solutions to fix these crises.
Have your say
Share your comments on the OMA's Prescription for Ontario

Reduce wait times and the backlog of services
Sick patients don’t have time to wait, but the COVID-19 pandemic has created a backlog of almost 22 million medical services — more than one patient service for every Ontarian, from the youngest to the oldest.
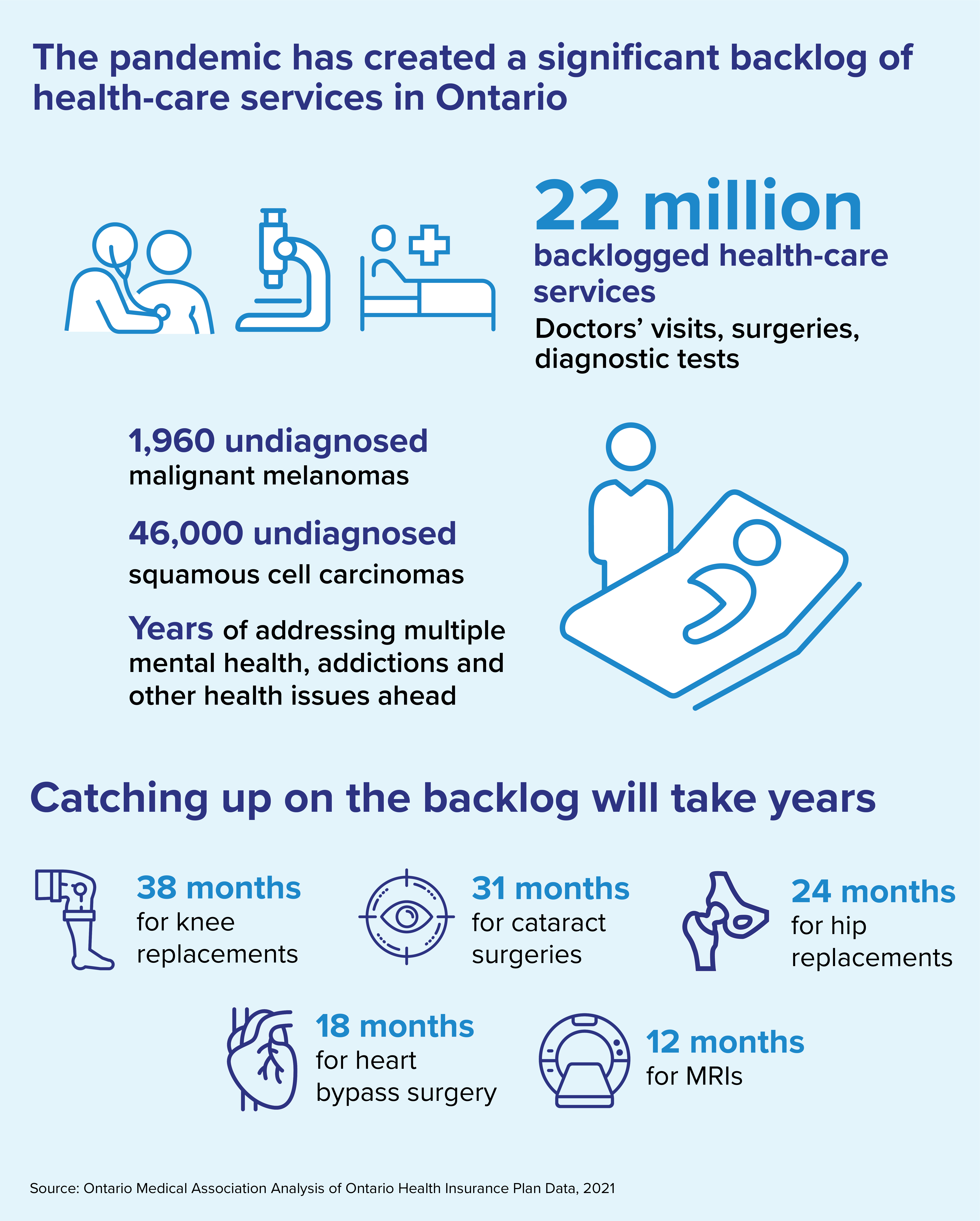
The COVID-19 pandemic has created a backlog of almost 22 million medical services — more than one patient service for every Ontarian, from the youngest to the oldest.
These delayed services include preventive care, cancer screening, surgeries and procedures, routine immunizations and diagnostic tests such as MRIs and CT scans, mammograms and colonoscopies. Doctors are seeing patients sicker than they ought to be because of serious conditions left undetected or untreated during the pandemic.
Sick patients don’t have time to wait. However, focusing on the pandemic backlog alone ignores the bigger problem. We can’t solve Ontario’s long-term problem of wait times and hallway medicine if the health-care system remains inefficient and disconnected.
Ontarians agree. Other than the pandemic, wait times is the issue most frequently selected — by 29 per cent of respondents — as the top priority for health care in the OMA’s online public survey.
Additionally, 21 per cent of Ontarians who responded to the survey selected “Wait times at our hospitals are too long and need to be reduced” as the statement that best represents their view on health-care delivery in their community.
A new model of care
Integrated Ambulatory Centres: A Three-Stage Approach to Addressing Ontario’s Critical Surgical and Procedural Wait Times calls for immediate attention to eliminate the pandemic backlog of health-care services and the creation of a new model of care called Integrated Ambulatory Centres.
Read the executive summary.
Read the full proposal.
Recommendations to reduce backlog and shorten wait times
- Provide adequate funding to address the backlog of services in hospitals and community clinics
- Evolve the model of surgical care delivery to include a greater portion of services delivered in community-based specialty settings outside of hospitals
- Ensure enough nurses and technologists to expand MRI and CT machine hours, and for ultrasound and mammography
- Greater efforts to educate young people about healthy lifestyles and disease prevention, including an adequately funded tobacco strategy, which will lead to better long-term health and reduce future stress on the system
- Expand the use of home remote monitoring programs to streamline pre- and post-surgical delivery
- Ensure sufficient health human resources to meet Ontario’s needs
- Enhance data collection and timely data sharing to support planning, measurement and evaluation
- Better integration of health-care service provision with public health and other services, including but not limited to palliative care, long-term care, home care and community care
“Cancer isn’t waiting for the pandemic to be over.” — Dr. Timothy Asmis, chair, OMA Section on Hematology and Medical Oncology, Ottawa
Fixing doctor shortages
Ontario continues to experience doctor shortages in many regions — especially in the north and remote and rural communities — and in certain specialties such as family medicine, emergency medicine and anesthesia. This is being felt by Ontarians.
Twenty-six per cent of respondents to the OMA’s online public survey chose “We don’t have enough doctors” as the statement that best represents their view on health-care delivery in their community.
Ontario’s doctors know that prevention is key to long-term health and positive outcomes. The public also recognizes this, with 32 per cent of survey respondents choosing “We need to do more to keep people healthy and out of hospitals and doctors’ offices” as the statement that best represents their view on health care delivery in their community. Respondents in Toronto and the Greater Toronto Area particularly hold this view
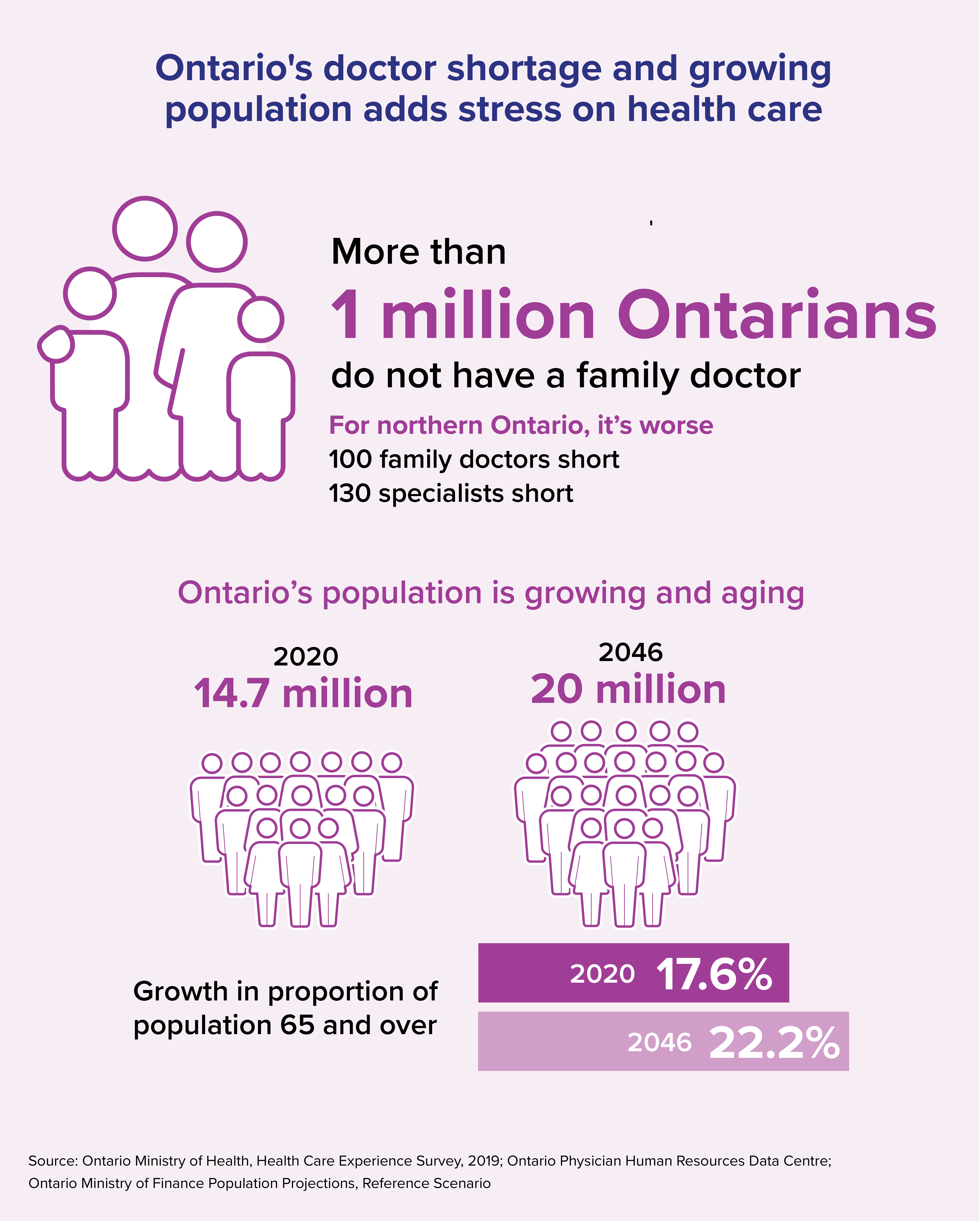
Primary care is the foundation of Ontario’s health-care system. But at least one million Ontarians don’t have a family doctor. Family doctors help patients stay healthy, prevent disease by identifying risk factors, manage chronic disease and get their patients access to specialists and other health-care services when needed.
Without access to doctors, many patients needlessly worry and suffer. We need robust data about our physician workforce and we need to use that data wisely to plan for our future population needs. We also need to support doctors so that all patients can get equitable and timely access to the care they need.
Recommendations to address unequal supply and distribution of doctors
- Create a detailed analysis, based on high-quality data, that accounts for the types and distribution of doctors to meet population needs
- Establish a set of best practices around physician supports to help ensure Ontario has the right doctors in the right places at the right times
- Use best evidence regarding forecasted population need, increasing the number of medical student and residency positions
- Support students from remote, rural and racialized communities to go to medical school aligned with populations in need
- “Let doctors be doctors” whereby they spend more time with patients doing the things that only doctors can do and less time on paperwork or other tasks
- Help doctors trained in other jurisdictions become qualified to practise here
- Invest in more training and educational supports for practising doctors

Expand mental health and addiction services in the community
In any given year before the pandemic, one in five people in Canada experienced a mental health problem or illness. Doctors continue to provide excellent care, but they do not have enough hours in a day to accommodate the tsunami of new patients.

Improve home care and other community care
In 2019-20, there were 1.3 million hospital bed days used by alternate level of care patients. This creates a major bottleneck that increases surgical wait times, leads to hallway medicine and doesn’t make financial sense.

Strengthen public health and pandemic preparedness
Public health defends the health of the entire community. Not only does it help combat pandemics and other public emergencies, but a strong system led by specially trained doctors preserves health and prevents illness every day.

Give every patient a team of health-care providers and link them digitally
Patients are healthier, have fewer hospital admissions and are more satisfied when they have a team of care providers, including not only family doctors and specialists, but also nurses, dietitians, physiotherapists and others.

Improve access to care in northern Ontario
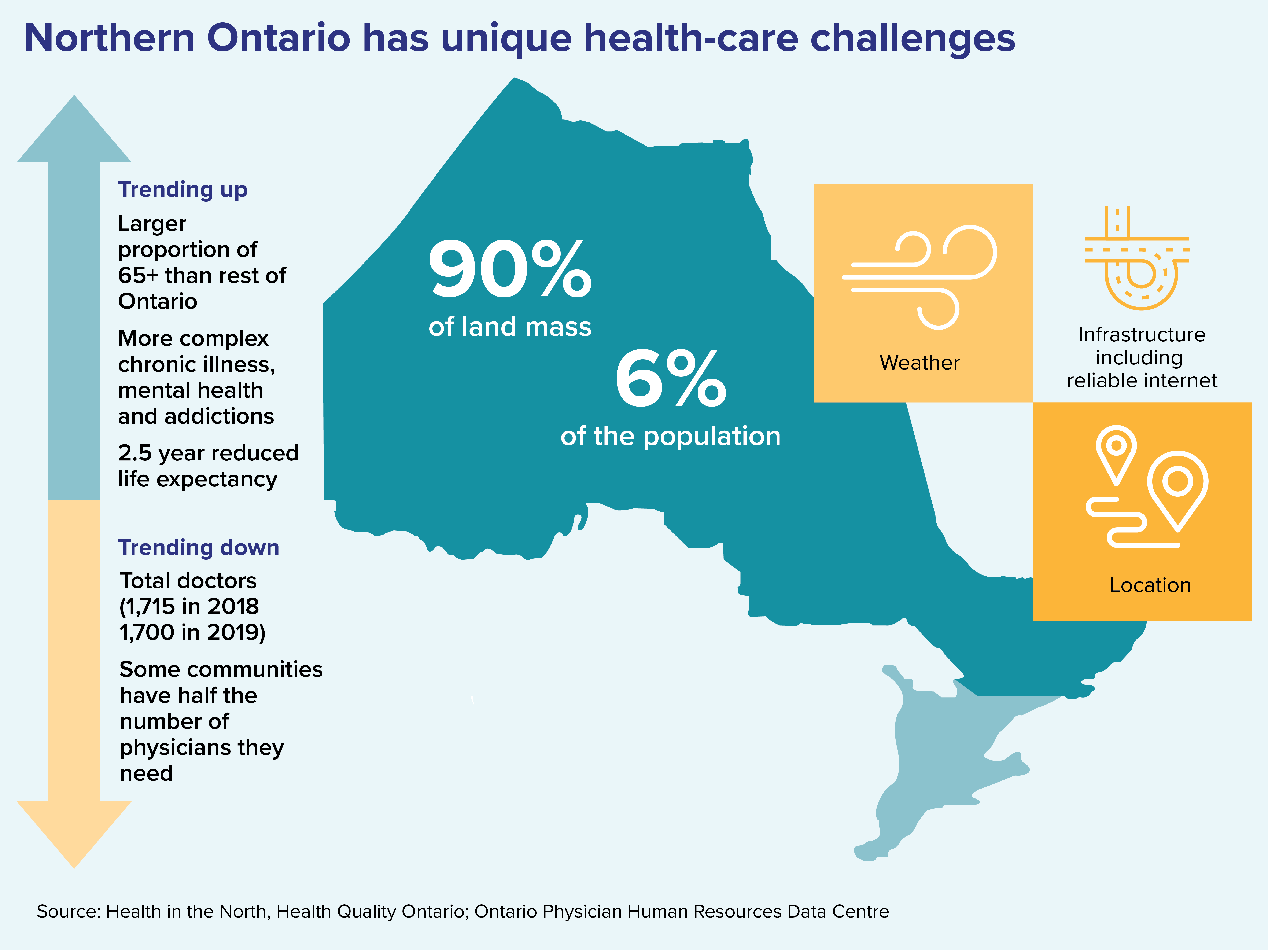
There is a shortage of doctors and health-care professionals in northern Ontario, and physical access to care and services is often hampered by weather, transportation and sheer distance. But it's crucial to the health and vibrancy of these communities.
Northern Ontario makes up almost 90 per cent of Ontario’s landmass but contains only six per cent of its population. Equitable access to health care in northern Ontario is a unique challenge, requiring unique solutions.
There is a shortage of doctors and health-care professionals in many northern communities, and physical access to care and services is often hampered by weather, transportation infrastructure and sheer distance. However, access to health care ensures healthy populations, which is crucial to the economic health and vibrancy of rural and remote communities.
Virtual care is limited by lack of high-speed internet and unreliable connectivity. It’s also hard to stay healthy when access to transportation, affordable food and secure housing are so limited. The social determinants of health must be addressed.
“Social isolation of Indigenous communities in the North, and the inequities experienced by Indigenous Peoples have been exacerbated by the pandemic. Our inequity bathtub in northern Ontario was nine-tenths full before COVID, and now it is overflowing.” – Dr. Sarita Verma, president of the Northern Ontario School of Medicine, Thunder Bay
Recommendations to improve health care in northern Ontario
- That patients have equitable of access to care in their own communities
- Review and update incentives and supports for physicians and allied health-care workers to practise in northern Ontario, and other communities that are chronically underserviced
- Focus on education, training, innovation and opportunities for collaborative care to address physician (health-provider) shortages in remote communities
- Create resourced opportunities for specialist and subspecialist trainees to undertake electives and core rotations in the North
- Give medical students and residents the skills and opportunities they need to be confident in choosing rural and remote practices
- Focus on innovative culturally sensitive education and training opportunities addressing physician and other health-provider shortages in rural and remote communities
- Focus on the profound and disproportionate impact of the opioid crisis and mental health issues in northern Ontario
- More social workers, mental health and addiction care providers and resources for children’s mental health
- Enhance internet connectivity in remote areas to support virtual care, keeping in mind that virtual care will not solve health human resources problems in northern Ontario and should not replace in-person care
- A recognition of the specific need for local access to culturally safe and linguistically appropriate health care for northern Ontario’s francophone population and Indigenous Peoples
- A collaborative partnership with Indigenous Services Canada and Health Canada to address issues of safe drinking water, and adequacy of health-care facilities and resources in Indigenous communities
- Using a harm reduction, anti oppressive lens, address the education gaps in Indigenous communities and non-Indigenous communities, as health is directly affected by education
Related stories from the Ontario Medical Review
Fall 2021 issue
Physicians teetering on 'edge of a cliff'
Fall 2021 issue