
FHO+: Continuity of care measure
Continuity of care remains an important goal of the FHO model. The FHO+ model will include a new continuity of care measure and accountability process linked to capitation.
Key takeaways
About the measure:
- The accountability measure counts in-basket visits only because capitation payments are for these services
- Visits that include one or more in-basket fee services are counted as ‘1’ visit
- Only visits to family physicians (OHIP specialty ‘00’) are counted, not visit to other specialties or professions
- The measure is calculated across your roster at the physician level, not at the group level
- You will receive a new report with your roster’s continuity of care rate every month
- You will continue to receive your outside use report
- If your roster is below 75 per cent for any quarter, you will receive a notification by email from the ministry two quarters later
About the financial adjustment:
- A financial adjustment is only applied if both of the two related measurement quarters are below 75 per cent. Related measurement quarters are three quarters apart (Qx + 3).
- The value of the financial adjustment is 15 per cent of the base capitation payments made to you in the first of those two related measurement quarters
- The adjustment is applied two quarters after the second related measurement quarter that is below 75 per cent, spread evenly over the last two months of the quarter
- This process resets every quarter and continues on a rolling basis
A note on terminology
Previous versions of this web page used the term 'discount' to describe the capitation adjustment. This language was updated to match the term used in the FHO contract.
Continuity of care video series
Learn about the value, timing and real-life scenarios behind capitation adjustments
In-basket fee codes
Overview
The new continuity of care measure will calculate the proportion of in-basket visits that are provided to your rostered patients (including long-term care enrolled patients) by you, a physician in your FHO or another physician that the ministry deems an “Acceptable Provider” (for example, a focused practice physician) versus in-basket visits provided to your rostered patients by any family physician (OHIP specialty code ‘00’). Please note that your roster of LTC-enrolled patients will be measured using the LTC basket of fee codes.
The continuity of care threshold was set at 75 per cent by the arbitrator – this means 75 per cent of in-basket primary care visits in a quarter should be provided to your rostered patients by you or other acceptable providers. Currently, the vast majority of FHO physicians (86 per cent) are meeting this continuity threshold, and another nine per cent of FHO physicians are within 10 per cent of doing so.
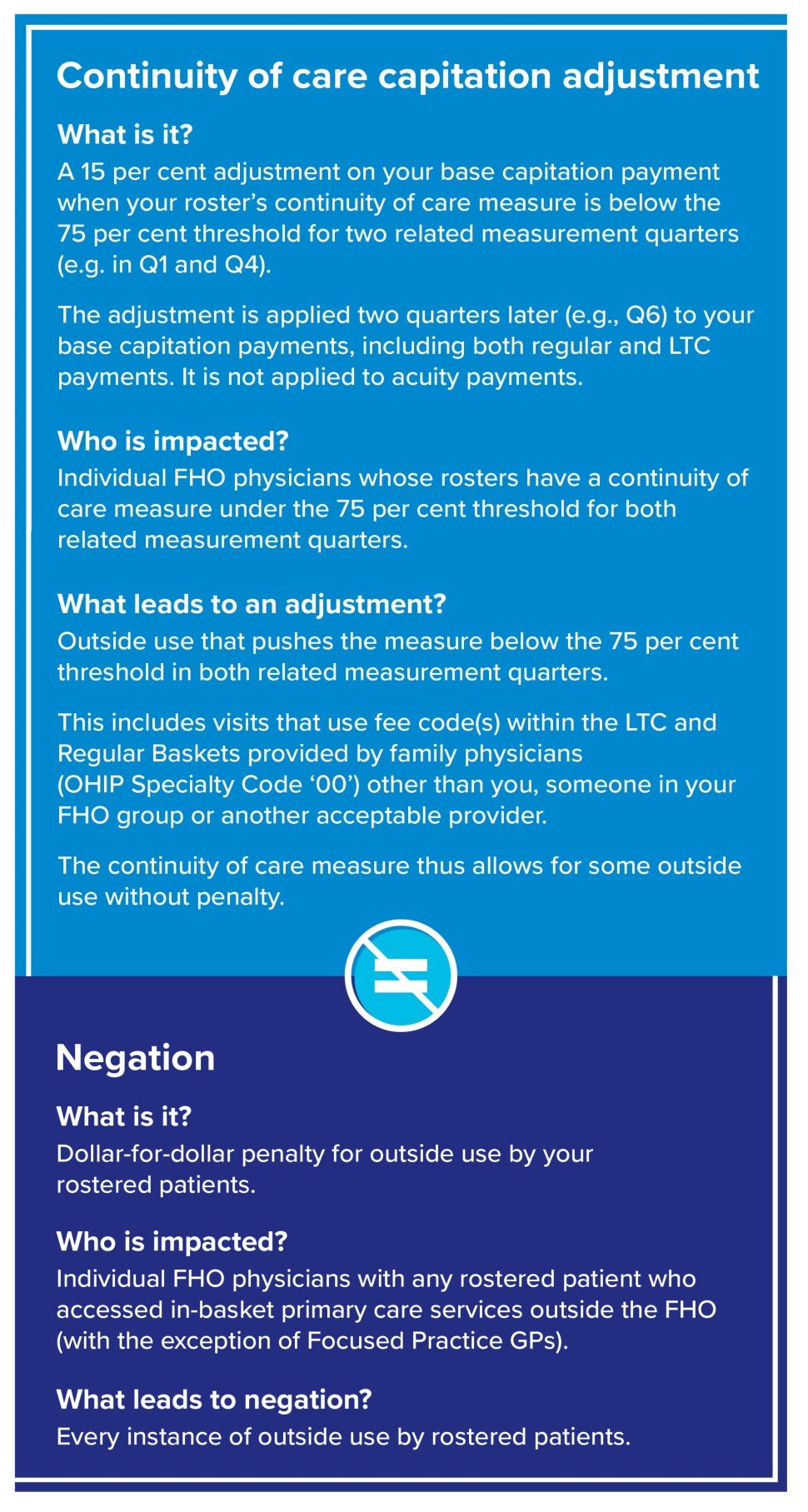
As with the previous FHO model, physicians will be held accountable for providing continuity of care. If the minimum continuity of care threshold is met, there will be no financial consequence. However, FHO physicians whose rosters fall below the continuity threshold in two related measurement quarters will have a 15 per cent adjustment applied to their base capitation payment.
The continuity of care measure will take effect on April 1, 2026, the start date of the new FHO+ model.
How it is calculated
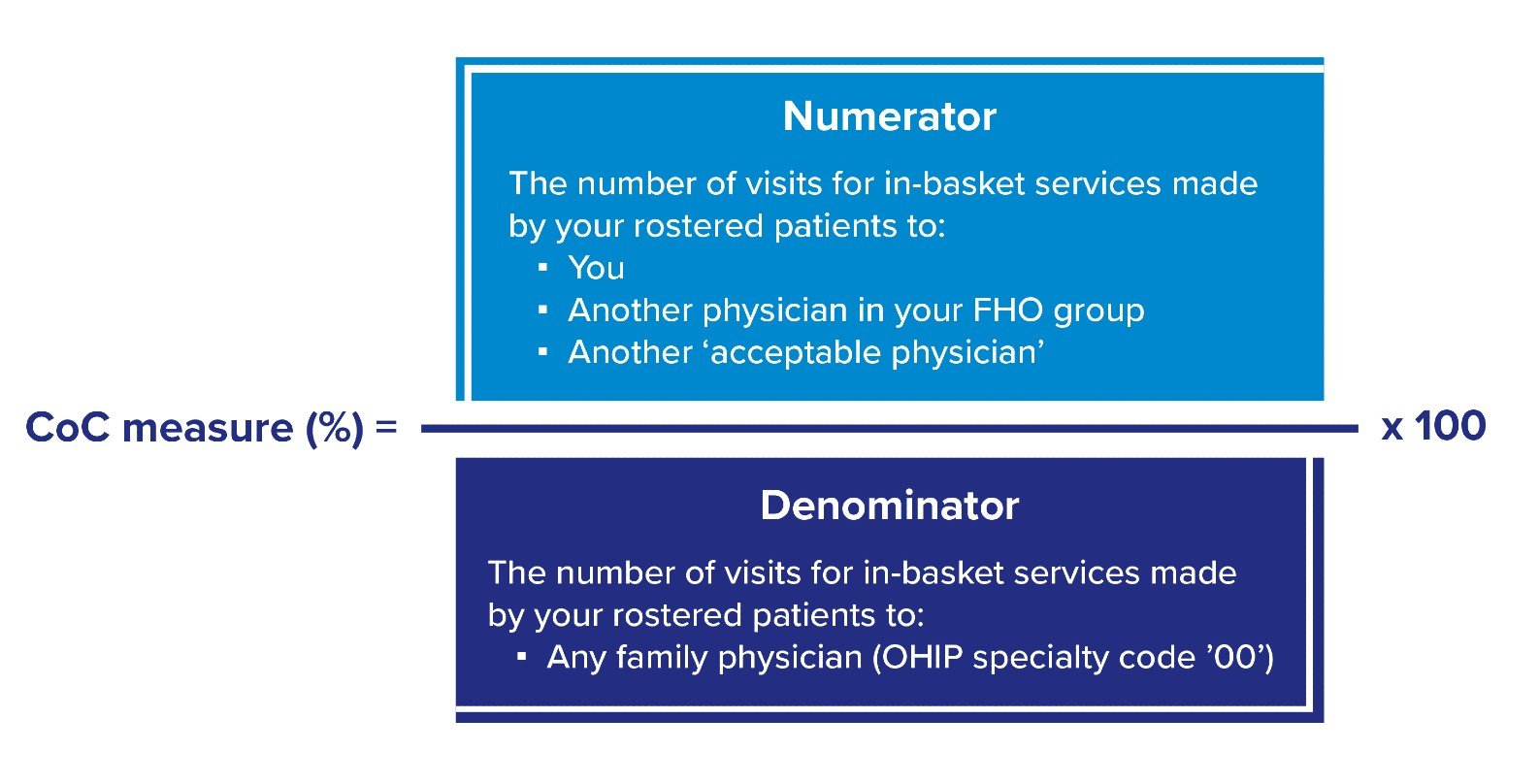
The OMA and the Ministry of Health have agreed on how the continuity of care measure will be calculated. The measure will reflect in-basket visits for rostered patients, including LTC rostered patients, using the respective baskets. Visits that include multiple in-basket services will be counted as one visit. The continuity of care measure will be calculated as a percentage for each FHO physician based on their rostered patients. It is calculated for the entire roster each quarter. The calculation is as follows:
What is not included in the measure
The continuity of care measure is intended to provide accountability for capitation payments and only measures in-basket services provided by Ontario family physicians.
As such, the continuity of care measure does not count:
- Any out-of-basket services, such as prenatal care P004, diabetes management K030, sexually transmitted disease management K028, etc.
- Care provided to your patients by non-physicians, such as nurse practitioners. However, having NPs and other professionals in your practice can provide your roster with overall better access to care, thus decreasing outside use that could otherwise impact your continuity of care measure.
- Virtual care provided to your patients by physicians who are out-of-province or who offer pay-out-of-pocket services
- Additional clinical tasks, such as answering patient questions by secure email
Reporting
The ministry will provide a new standalone monthly report on continuity of care. The report will be based on the previous month’s OHIP claims, and will include:
- The number of visits for in-basket services to acceptable physicians (numerator)
- The number of visits for in-basket services to any family physician (denominator)
- Your continuity of care percentage
Eventually, you will receive this report through your Medical Claims Electronic Data Transfer (MCEDT) account. However, for the first year, the continuity of care report will not be available through MCEDT; instead, the ministry will send it via email to your FHO Lead and they will share it with you. This alternative distribution method will be temporary.
You will continue to receive your outside use report, in addition to the new continuity of care report.
Accountability for continuity of care
The arbitrator concluded that there should be a modest financial consequence for FHO physicians who fall below the minimum continuity of care threshold of 75 per cent. Note that the vast majority of FHO physicians (86 per cent) are meeting this continuity threshold, so will not face any financial consequences. For physician rosters not meeting the continuity threshold, here’s how accountability will work
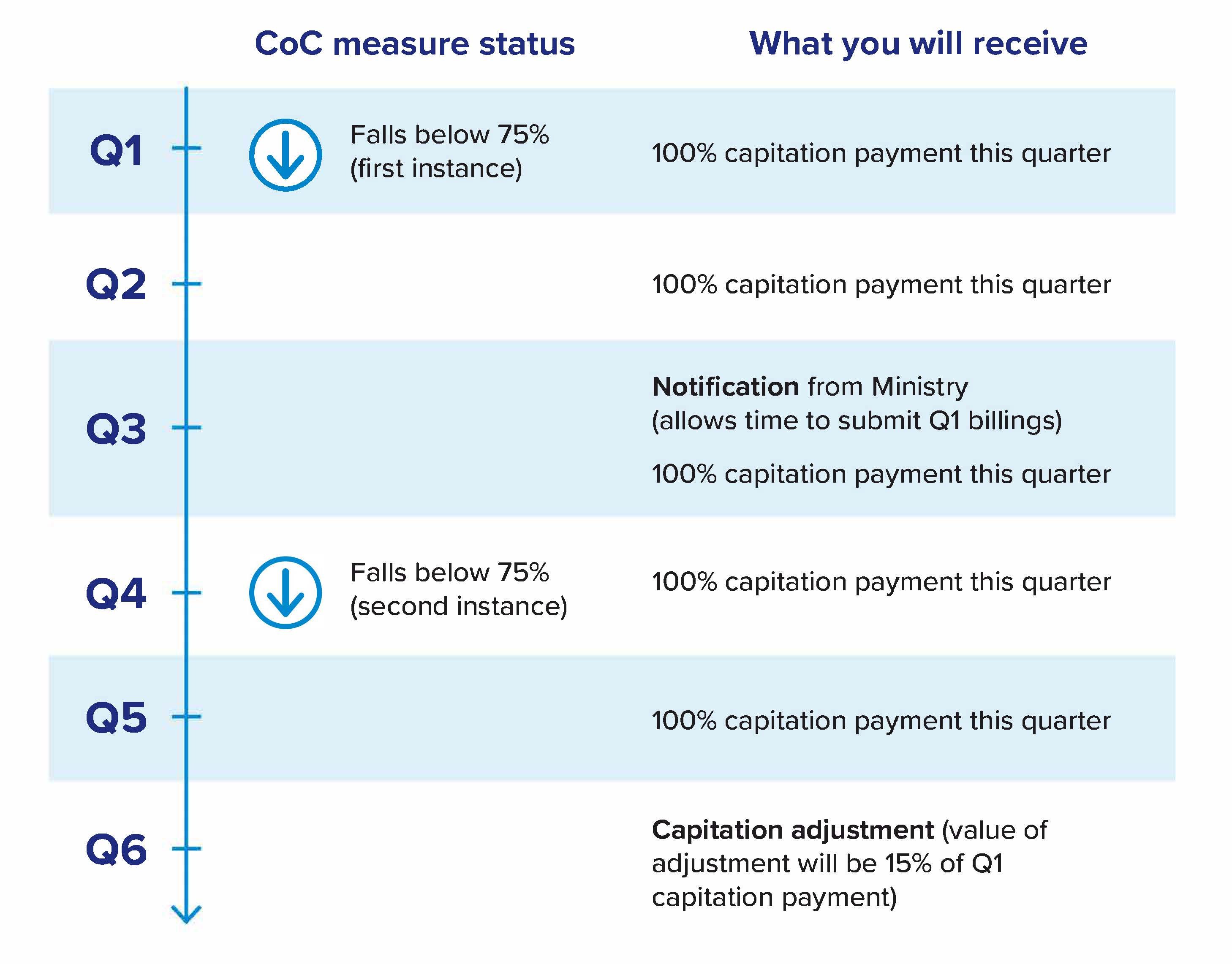
For the first quarter of your roster not meeting the continuity of care threshold of 75 per cent, you will be notified by the ministry. Because you have up to three months from the date of service to submit billings, a notification for Q1 will come early in Q3. There is no financial consequence for being under the continuity threshold for a single quarter. The notification serves as an opportunity to course correct.
If your roster does not meet the 75 per cent continuity of care threshold for the quarter following notification (Q4) – a second quarter of your roster being below 75 per cent – 15 per cent of what was paid to you in Q1 will be subtracted from your Q6 capitation payment. This adjustment will be applied to your total capitation payments (including both regular and LTC capitation payments).
How the continuity of care adjustment differs from negation
Negation is a dollar-for-dollar reduction each time a rostered patient seeks care outside of your FHO for in-basket services.
Under negation, outside use reduces the amount of the access bonus you receive by the dollar value of the fee code used for the visit.
This differs from the continuity of care adjustment, which is applied to the capitation payment only when the continuity of care measure for your roster falls below the continuity threshold of 75 per cent in two related measurement quarters.
Note that negation and the access bonus will remain in Family Health Networks and Blended Salary Models. The continuity of care measure does not apply to these models.
The continuity of care measure makes more allowances for the realities of how patients access health care and allows more outside use than negation. The vast majority of FHO physicians (86 per cent) will not face financial consequences since their roster is currently meeting the 75 per cent continuity threshold. For physicians whose rosters are not meeting the continuity threshold, there is still an opportunity to improve their continuity of care measure and avoid future financial consequences.
Avoid comparisons with the access bonus
Your continuity of care measure will not be the same as your access bonus capture rate. For example, if you typically receive 65 per cent of your access bonus, that does not mean that your continuity of care measure will be 65 per cent. The continuity of care measure is calculated differently. It includes your rostered patients’ visits to your group and to other acceptable providers as part of continuity of care and counts the visits towards your continuity of care percentage. Some of these, like Emergency Department or hospital visits that used in-basket fee codes, were previously considered as outside use.