
FHO+: Frequently asked questions
The following questions and answers focus on the new FHO+ model, including hourly rates, continuity of care, and patient attachment bonus.
FHO+ model
FHO+ is a modernized version of the Family Health Organization model that adds new incentives to support comprehensive, longitudinal family medicine, including a new hourly payment to recognize the time physicians spend on direct care, indirect care, and administrative work. It also includes higher shadow billing rates, increased after-hours premiums, and new unattached patient fees, including patient attachment bonuses, among other things.
FHO+ is effective as of April 1, 2026. Existing FHOs transitioned to FHO+ on that date after signing the updated FHO contract. New FHOs will join the FHO+ model upon signing the contract.
Hourly rate
You must maintain records of your total time spent in each category per day: direct patient care (both direct care in-person or virtually provided in-office or by video provided out-of-office and direct care telephone-based out-of-office), indirect patient care and clinical administration. Only daily duration needs to be recorded; start and stop times are not required at the patient level. Documentation does not need to be at the patient level. This applies to your enrolled patients. Hourly rates are not available for non-rostered patients.
Indirect care and clinical administration records must include a summary description of the activities associated with each category. An example of a summary description for indirect care could be: “charting, reviewing results/reports in inbox, making referrals.”
OntarioMD will provide resources to support you in documenting your hours ahead of April 1, 2026 that you can choose to use.
Yes, if you are going to submit a claim for the hourly rate, you must have documented hours for that day. Each hourly rate claim needs to have the date the services were performed on. Claims do not necessarily need to be submitted daily, but you should track your activities every day.
If you did not do any FHO+-related work a particular day and therefore have zero hours in any category, you do not need to document that day.
No. Since hourly rate billing is not at the patient level, there is no need to track at the patient level.
No, you do not need to specify the time you spend on each individual activity for indirect care and clinical administration. However, you do need to indicate which activities you did for these categories in a particular day if you claim for the respective hourly rate. For example, for indirect care, “charting, reviewing results/reports in inbox, making referrals.”
You can use your own discretion to separate out the time you spend on direct care, indirect care and clinical administration for non-rostered patients. This is necessary since you cannot bill the hourly rate for non-rostered patients.
An example of a summary description for indirect care could be: “charting, reviewing results/reports in inbox, making referrals.”
No, you cannot bill for hourly work that you did not personally render.
No.
Clinical insured services (e.g., medically necessary) do not attract HST. As the clinical administration hourly rate is for management of your patient panel and practice, it will be exempt from HST.
Video-based virtual care provided out-of-office is billed at $80/hour using code Q310 – Direct Patient Care – In-Person or Video.
Telephone virtual care provided out-of-office is billed at a rate of $68/hour using code Q311 – Direct Telephone-based Patient Care – Not in Office.
Yes, this counts as direct patient care, which is payable for time spent personally providing insured clinical services to rostered patients of the FHO group for in-person care and synchronous virtual care. This is billed at $80/hour (hourly rate) in addition to the applicable fee codes for the visit.
No. In this context, an office
is considered to be the usual family practice setting where your patients come to see you. If you do telephone care from your home office, this is billed at $68/hour (85 per cent of the hourly rate).
Yes, you can bill the hourly rate for teaching undergraduates, residents and fellows when it’s related to:
- At the bedside care: clinical teaching done concurrently with delivering patient care (this would be billed as Q310 – Direct Patient Care), or
- Case reviews and follow-up: patient-specific clinical teaching that arises from direct patient care (this would be billed as Q312 – Indirect Patient Care)
No. The hourly rate can only be billed once per hour, even if you are supervising more than one learner at the same time.
Yes, this is considered at the bedside
and you can bill the direct care hourly rate.
No, you cannot bill the direct care hourly rate for services provided by your learners unless you are directly supervising them at the same time as they provide direct care. However, if afterwards you carry out services that are included in the indirect hourly rate such as chart review, preparing referrals, etc., with your learner then the indirect hourly rate can be billed.
Yes. Patient panel management for the purpose of screening, interventions, disease management, and provision of care (e.g., mammograms, colon cancer screening, immunizations, diabetes management) would be considered eligible.
In summary, if it is for your panel population and a larger management issue of the practice, not on an individual basis, then it is eligible for the CAT hourly rate.
Yes. If you hire a locum to cover your FHO practice, the locum can bill and receive payment for the hourly rate when providing services to the FHO’s enrolled patients, provided the locum is registered through the proper channels with the FHO.
Starting April 1, 2026, payment for all hourly rate claims for registered locums will go to the FHO group account, as they are treated like fee-for-service claims. FHO groups should work with their locums to determine how payment of hourly rate claims will be made.
As of April 1, 2027, locums will have the option to select for payments to go either to themselves or the group, depending on how the FHO group has set up their payments. Locums should keep track of the hours they bill under each particular FHO so they have a record of this to reconcile their payments against.
Yes, you can bill the hourly rate for services you provide to LTC patients rostered using a Q202 (LTC roster fee code). However, travel time is excluded.
Your RA will show the total number of hours paid, but not the billing limits.
For the first year, April 1, 2026 to March 31, 2027, the hourly rates will be payable up to the daily maximum of 14 hours per day, and the monthly maximum of 240 hours per 28 days, pro-rated monthly. If you bill over these limits, your claim will be rejected. You can resubmit your claim to fall within the allowable limit.
In addition to the limit above, a maximum of 25 per cent of your total billable hours (averaged over 28 days) can be for indirect care and clinical administration (together), and five per cent of your total direct and indirect care hours (averaged over 28 days) can be for clinical administration. These limits will be applied retroactively and recovered if there is an overbilling in any given month.
Starting April 1, 2027, hourly claims will no longer be paid right away. Instead, they will be tracked and paid as a single monthly amount, after applying all limits (including the 25 per cent indirect care cap). You don’t need to worry about overbilling – the system will automatically calculate and adjust the payment for you.
OntarioMD will provide resources to support you in documenting your hours ahead of April 1, 2026, that you can choose to use.
Yes, the hourly rate payments will be a separate item on the RA and reported per code.
You can bill a maximum of 14 hours per day and 240 hours per 28 days, pro-rated monthly. Additionally, a maximum of 25% of your total billable hours can be for indirect care and clinical administration. In other words, up to 33 per cent of direct patient care hours can be used to bill for indirect care and clinical administration.
Five per cent of your total direct care and indirect care hours, averaged over 28 days, can be for clinical administration.
The maximum you can bill per month is 240 hours per 28 days, pro-rated monthly. This works out to the maximums below, depending on the number of days in the month:
| Month | Monthly limit |
| 28 days | 240 hours |
| 29 days | 248.6 hours |
| 30 days | 257.1 hours |
| 31 days | 265.7 hours |
During year one of implementation, the only limit in place within the ministry’s billing system will be the maximum 14 hours a day and the prorated monthly limit of 240 hours per 28 days (pro-rated monthly). A physician can submit above this limit, however, if they do, the hours over the limit will be rejected.
The 25 per cent indirect and five per cent CAT will not have a limit in the ministry’s billing system until year two. If a physician goes over these two percentages, they will be paid and the ministry will reconcile any overpayment at a later date.
Reports can be batched, however each code must be attached to a specific date.
They can be submitted separately.
For EMR setup and subsequent billing submission, the billing codes should be assigned a value of the appropriate hourly rate divided into four 15-minute increments.
The value per unit for each fee code is:
- Q310 – Direct Patient Care – In-Person or Video: $20/unit
- Q311 – Direct Telephone-based Patient Care – Not in Office: $17/unit
- Q312 – Indirect Patient Care: $20/unit
- Q313 – Clinical Administration Time: $20/unit
Physicians should bill for the value of the codes based on the number of units billed. For example, 1 hour (4 units) of Q310 should be billed at $80.
Similar to the Preventive Care Bonus, it is important to ensure your EMR is configured to submit claims that are not linked to a patient health card number.
If you need to add an hour, bill the additional unit as needed and the system will add it, as long as it stays within the daily/monthly limits.
To revise an overbilled amount, submit an RA inquiry to adjust the previously submitted claim.
- The health number, version code and birthdate fields on the claim must be left blank.
- When an hourly code is submitted without a blank health number field the claim will reject ‘VHB – No HN required for HSC.’
- When an hourly code is submitted without a blank version code field the claim will reject ‘VHB – No HN required for HSC.’
- When an hourly code is submitted without a blank birthdate field the claim will reject ‘VH1 – Invalid Health Number.’
- The service date for any hourly rate billing code must reflect the actual date on which the hourly activity was performed.
Continuity of Care
The Continuity of Care measure counts the number of visits for any in-basket services (e.g., assessments, procedures, etc.) provided to your rostered patients, including both regular and long-term care patients.
The numerator is the number of visits for in-basket services provided by you, another physician within your FHO or another acceptable physician. The denominator is all visits for in-basket services made by your rostered patients to any family physician (OHIP specialty "00").
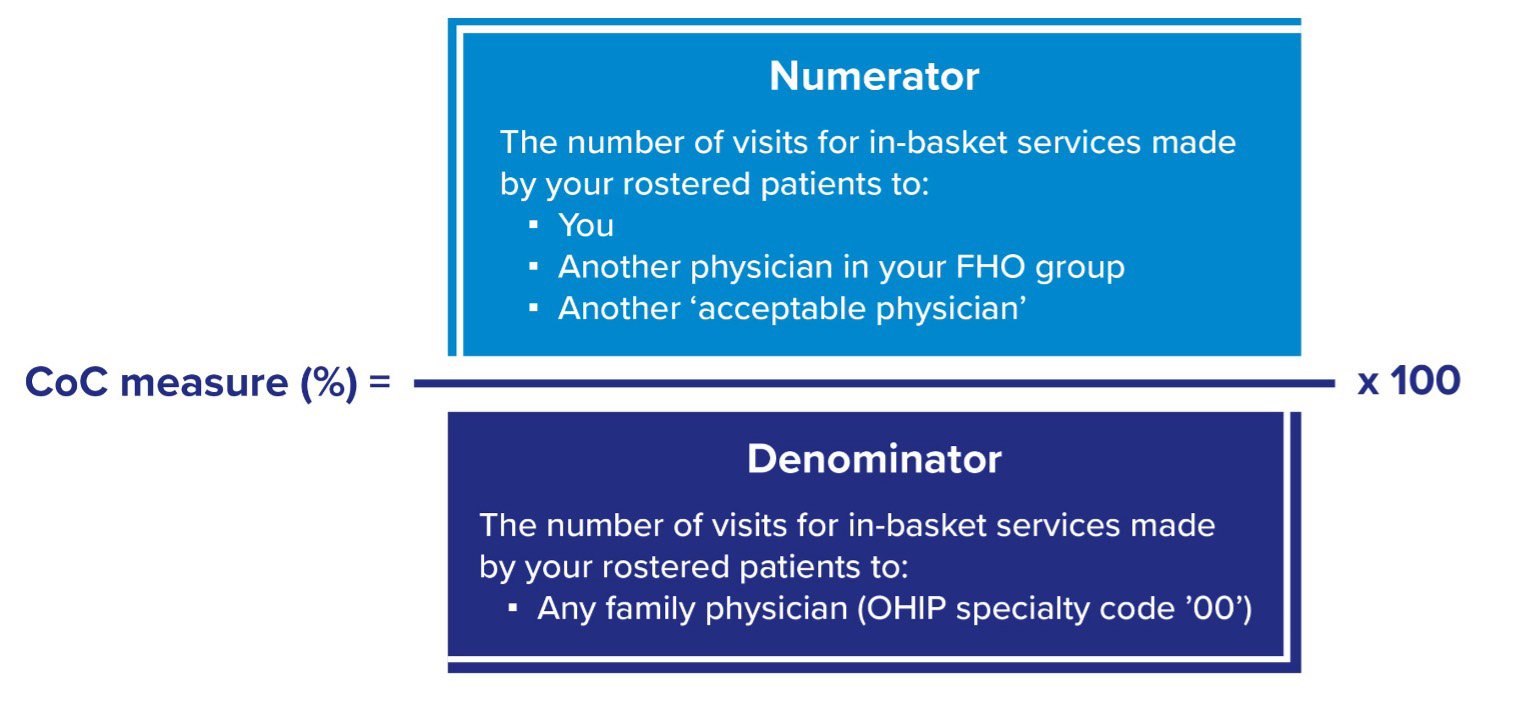
The Continuity of Care measure counts visits for any in-basket services (e.g., assessments, procedures, etc.) provided to rostered patients by family physicians. A single visit with multiple in-basket fee codes counts as one visit.
Examples:
- A visit that includes multiple in-basket codes, such as an intermediate assessment and a pap smear, is counted as a single visit for the Continuity of Care measure
- A visit for a G848 Varicella immunization only (no assessment) is counted as a single visit for the Continuity of Care measure
The Continuity of Care measure is calculated across your full roster, not per enrolled patient.
Each quarter, the ministry calculates a single percentage for each individual FHO physician based on all of their rostered patients, including both regular and long-term care patients.
The threshold for the Continuity of Care measure is 75 per cent. That means, for a given quarter, at least 75 per cent of your rostered patients’ visits for in-basket services should be to you, another physician in your FHO, or to another acceptable physician.
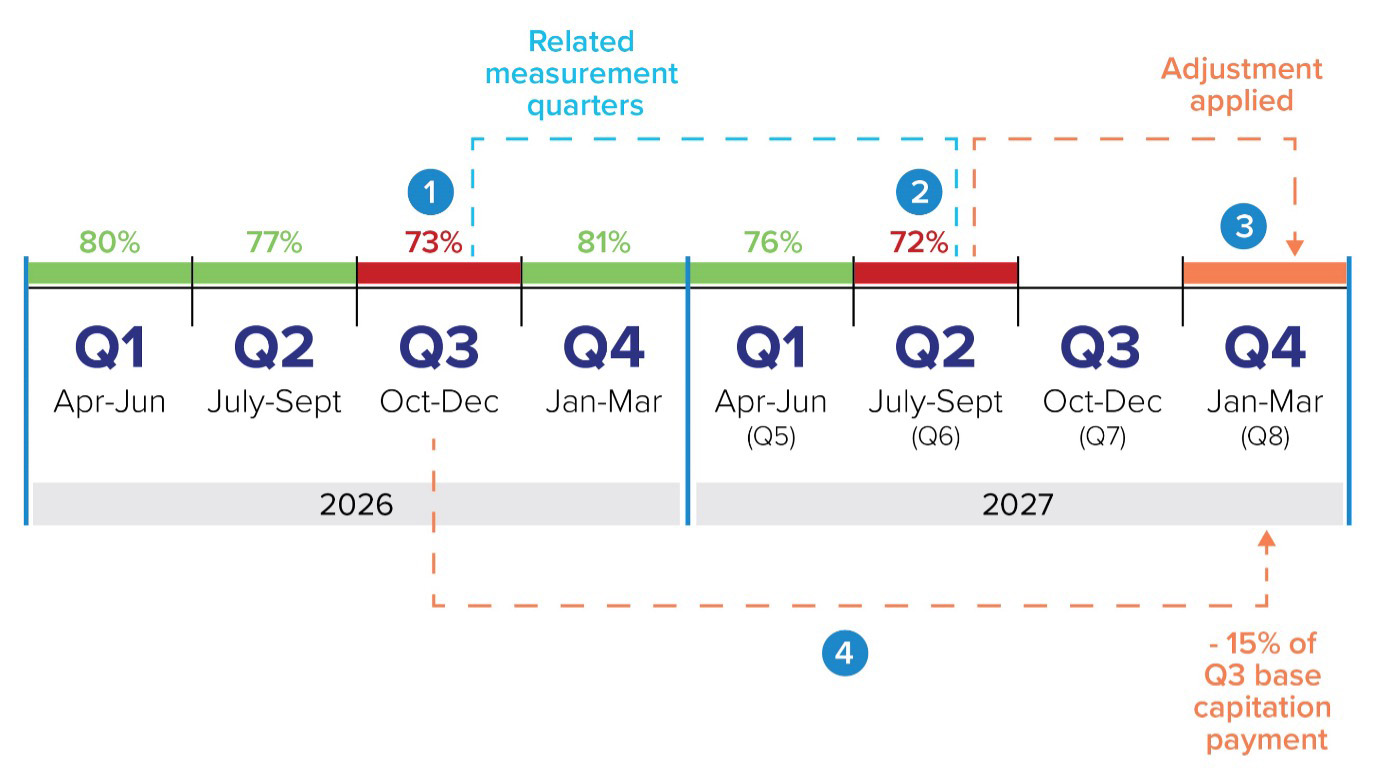
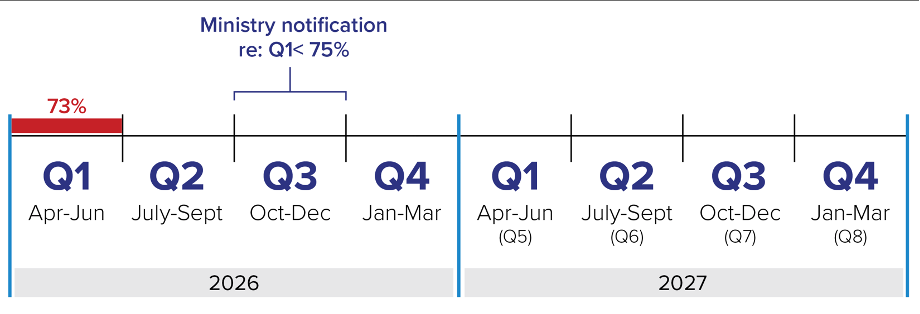
If a FHO physician’s roster is below the 75 per cent threshold for both related measurement quarters, an adjustment will be made to a future capitation payment. The value of the adjustment is 15 per cent of the base capitation payments made to you in the first of the two related measurement quarters.
Here is the step-by-step breakdown:
- Steps 1 and 2: Related measurement quarters are three quarters apart. If they are both under 75 per cent, a capitation payment adjustment will be applied
- Step 3: If applicable, the capitation payment adjustment is made two quarters after the second measurement quarter.
- Step 4: The value of the adjustment is 15 per cent of the value of the base capitation payments made to you in the first of the two related measurement quarters.
Remember: a capitation adjustment is only applied if BOTH related measurement quarters are below 75 per cent.
A related measurement quarter is essentially a pair of quarters (three quarters apart).
For example, Q1 measurements are related to Q4 measurements. Q2 is related to Q5, and so on. For an adjustment to be applied, BOTH related measurement quarters must be below 75 per cent.
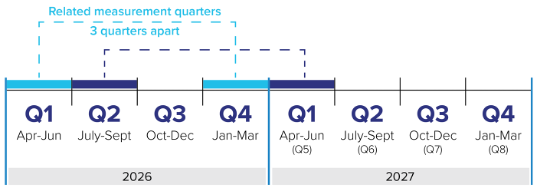
A financial consequence applies if a roster falls below the 75 per cent continuity threshold in both of the related measurement quarters. Related measurement quarters are three quarters apart.
The adjustment is applied against base rate payments for the first related measurement quarter, but it is done two quarters after the second related measurement quarter that is under the 75 per cent continuity threshold.
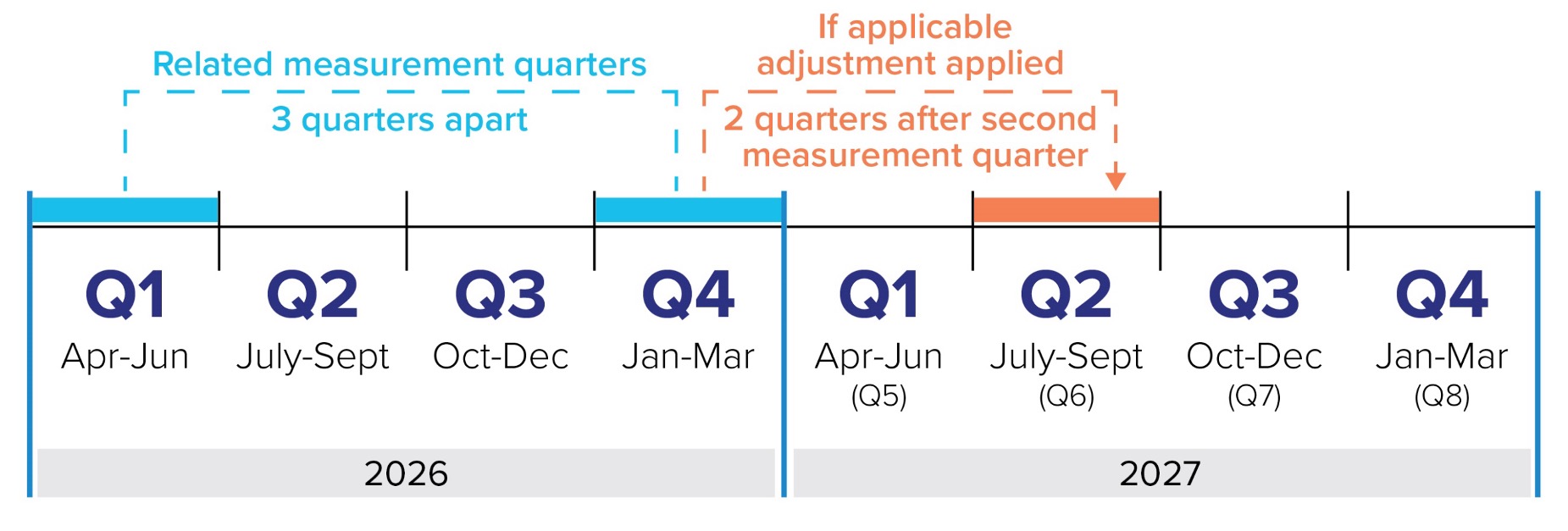
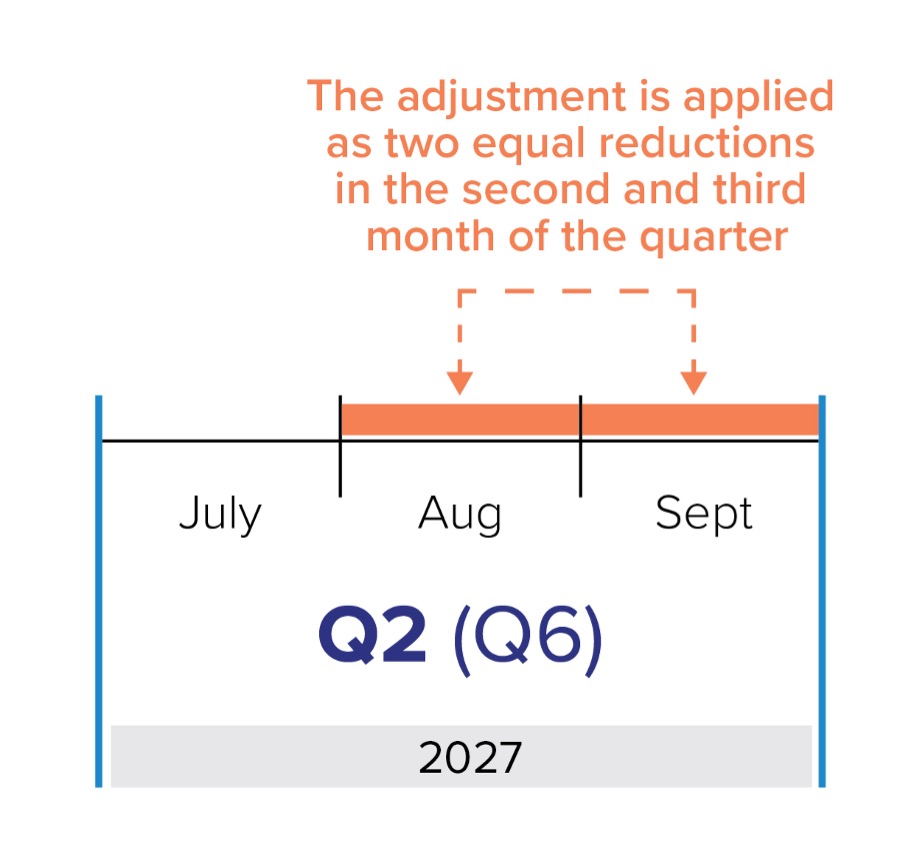
The adjustment will be applied as two equal amounts, subtracted from the second and third month of the adjustment quarter (i.e. two quarters after the second related measurement quarter).
For example, if your Q1 and Q4 are below 75 per cent, a discount will apply in Q6. The value of the adjustment is 15 per cent of the capitation payments paid to you in Q1. This amount will be divided into two and subtracted from your August and September payments (the second and third months of Q6).
Acceptable physicians include:
- You, the family doctor, they are rostered to;
- Another physician in your FHO group, including other FHO signatories, income stabilization physicians and locums registered to the group;
- Another “acceptable provider,” defined as a family physician using the "00" specialty code and is a:
- Designated GP focused practice physician (including GP psychotherapy) for in-basket visits using fee or diagnostic codes identified for their area of practice
- HIV or Care of Elderly COE physician billing in-basket fee codes
- Physician providing in-basket visits that take place in an ED and hospital as identified by a master hospital number, including special visits to an ED, using codes K990-K999, H980-H981, H984-H989
- Physician billing oculo-visual visits using fee codes A110A and A112A
Yes, the current outside use report will still be available on a monthly basis.
In addition, the ministry will provide a new standalone monthly continuity of care report. It will show your roster’s continuity of care measure for the previous month, using available claims data. Delivery of this report will start in May 2026.
Physicians will be able to monitor their performance through the new standalone monthly Continuity of Care report. Real-time calculations will not be available.
We will provide a sample report when we receive it from the ministry.
Yes. Physicians whose rosters fall below the 75 per cent threshold for the first quarter will be notified by the ministry via email.
The notification will come in the quarter following billing reconciliation, that is: two quarters after the quarter in question. This allows physicians three months to submit their OHIP billings before the ministry evaluates a given quarter.
The notification serves as an opportunity to course correct.
All FHO physicians will continue to receive their outside use report.
The notification will be sent via email from the Ministry of Health. It will be sent to you and your FHO lead physician will be CC’d.
The ministry will use the email address you have on file with them. Therefore, it’s important to ensure the ministry has your correct email address. When you sign the FHO Physician Declaration form, email address is one of the fields included; it’s in your best interest to sign that as soon as possible so the ministry has your current contact information.
If you need to update your email address with the ministry, please email them at primarycareinquiries@ontario.ca.
It applies to base capitation payments for all enrolled patients, not just those with outside use. The adjustment does not apply to acuity payments.
When two related measurement quarters are below the 75 per cent continuity threshold, the value of the adjustment is 15 per cent of the base capitation payments made to you for all of your rostered patients in the first of the two related measurement quarters. For example, for the related measurement quarters Q1 and Q4, the adjustment will be 15 per cent of the value of the payments made to you in Q1.
No. The “clock” resets each quarter. If your continuity of care improves and is above the 75 per cent continuity threshold in future quarters, you can avoid future financial consequences.
Not necessarily. The continuity of care measure is not the same as the access bonus capture rate. The two are calculated differently.
In-basket codes that are billed by a family physician working in a hospital or ER count toward both your numerator and denominator, and therefore will not negatively impact your overall Continuity of Care measure.
Family physicians working in an ER or another hospital setting submit their billings together with a master hospital number. This will identify them as part of the group of acceptable physicians that makes up the numerator of the Continuity of Care measure. Therefore, if they bill any in-basket codes for your rostered patients, this will count toward your Continuity of Care measure.
This will be captured by any in-basket visits that take place in the Emergency Department or elsewhere in a hospital identified by a master hospital number (including special visits to an emergency department: In-basket visits claimed with these codes: K990 to K999 series codes and H980 to H981; H984 to H989).
Yes. The numerator includes in-basket primary care visits provided in person or virtually by you, another member of your FHO, or an acceptable physician.
The denominator includes all visits for in-basket services to any family physician, in any setting.
However, visits by your rostered patients to a family physician in the ER or hospital for in-basket services are counted in the numerator. Therefore, visits for in-basket services to family physicians in an ER or hospital will count toward you and will improve your overall Continuity of Care measure.
Out-of-basket codes billed by any family physician, in any setting, do not count towards or against your Continuity of Care measure.
No. The Continuity of Care measure only evaluates continuity of care provided to your rostered patients by family physicians in Ontario – those billing with OHIP specialty code "00." Any other profession or type of physician is not counted in the measure.
If in-basket care is delegated to another team member (e.g., nurse or any other medical assistant), but billed by the physician, it counts as a physician-provided service.
As a reminder, the delegate may be any non-physician (e.g., physician assistant, nurse, nurse practitioner, etc.) who is properly trained to perform the procedure and where the procedure is one that is generally and historically accepted as a procedure which may be carried out by the medical assistant. In addition, the physician must be present in the office or clinic at the time the service is rendered unless an exception is met.**
In order for the delegated procedure to be eligible for payment by OHIP, the delegate must be employed by the physician. Employed means that there is an employment contract between the physician and the individual and Canada Revenue Agency receives income statements for tax purposes.
Note that all in-basket services provided in a single visit count as one visit for the purposes of the Continuity of Care measure. For example, if you see a patient for an assessment and delegate their flu shot to your nurse, that is counted as one visit.
**Physicians should review the Schedule of Benefits section on delegated procedures for the complete list of requirements for billing delegated procedures.
The Continuity of Care measure only measures care funded through capitation (i.e. in-basket care for rostered patients).
If the care is provided by a GP physician (OHIP specialty "00") in a hospital setting and they use a master hospital number to bill these hospital-based services, this will count toward your Continuity of Care measure (i.e. it will be counted in the numerator).
If palliative care is provided to your rostered patient outside of hospital, but by a focus-practice designated physician in palliative care, this will also count toward your Continuity of Care measure. This is because GP Focused Practice physicians are considered "acceptable providers."
Out-of-basket services (e.g., oncology, prenatal, diabetes care) are excluded from the Continuity of Care measure, which only evaluates the delivery of in-basket services. If your rostered patients see other physicians for care outside of the basket, it will not count against you.
In-basket care provided to your rostered patients by a locum registered to the FHO group count toward the numerator and support your Continuity of Care measure.
If you have a locum cover you, make sure they are properly registered to your FHO.
Visits provided by any physician within the same FHO group count toward the numerator and therefore support your Continuity of Care measure.
Visits provided by any physician within the same FHO group count toward the numerator and therefore support your Continuity of Care measure.
Out-of-basket services are excluded because capitation payments fund in-basket services only. The Continuity of Care measure is intended to provide accountability for capitation payments.
Provided that the in-basket visit is billed by the FHO physician, another physician in the FHO, or another acceptable physician, there will be no negative impact to your Continuity of Care measure.
Patient attachment bonus
There are several different bonuses available for attaching new patients. Some of them have been in effect for some time. Others are new, and effective as of July 1, 2025. All family medicine physicians in all patient enrolment models are entitled to claim these bonuses, subject to the rules that apply for each.
The fees range from $100 to $500, depending on:
- The age of the patient
- The physician’s office RIO score
- Whether the physician attaching (enrolling) the patient is a new graduate or established doctor
- Whether the patient is pregnant and/or has a newborn(s)
- Whether the patient is FIT positive (at risk for colorectal cancer)
- Whether the patient had a recent acute inpatient stay in hospital
- Whether the patient is from Health Care Connect and is determined to be complex and/or vulnerable
Criteria A to C apply to the new Patient Attachment Bonus. Categories D to F are separate bonuses for specific situations (e.g. the Health Care Connect bonus or the mother and newborn bonus).
Each code has specific requirements to fulfil, which may include the patient completing the appropriate patient declaration form. However, all newly enrolled patients and the physician must complete the Patient Enrolment and Consent to Release Personal Health Information form (“E/C Form”).
To bill, the physician must enrol the patient using the appropriate fee code (e.g. Q200A) and submit the relevant billing code for the patient attachment bonus. Only one patient attachment bonus code can be used per patient per group.
The patient must be new to the group and to the physician enrolling them. In other words, they have never been enrolled to any physician in your group at any point in time.
In addition, a new patient is one who has never had a family physician or one who does not currently have a family physician because:
- their family physician or the patient has moved to another community
- their family physician is no longer available due to illness, death, retirement or a change in practice type
- up until now the patient has not had or felt they needed a family physician
The patient declaration form requires the patient to declare that they satisfy at least one of the above criteria.
No. The patient attachment bonus does not apply to the scenario of taking over a physician’s entire roster (i.e. a batch roster transfer). In this situation, you cannot bill the patient attachment bonus for any patient on the batch roster.
All patient enrolment models are eligible for this fee code, including:
- BSM: Blended Salary Model
- CCM: Comprehensive Care Model
- FHG: Family Health Group
- FHN: Family Health Network
- FHO: Family Health Organization
- GHC: Group Health Centre
- GP-HIV: General Practitioner Specialized Model for HIV Patients
- GP Focus Care of the Elderly
- RNPGA: Rural and Northern Physician Group Agreement
- Rural Generalist Model
- Sioux Lookout Regional Physician Services Incorporated – also known as Sioux Lookout Agreement
- St. Joseph’s Primary Care Site at St. Joseph’s Hospital in Toronto
- WAHA: Weeneebayko Health Authority
There will be two fee codes for the new patient attachment bonus: one for existing physicians and one for new graduates. For each fee code, the ministry will adjust the payment based on the physician’s practice address (for the RIO score) and the patient’s age at the time of service.
Existing doctor in a patient enrolment model: fee code TBD
| Newly enrolled patient | RIO < 40 | RIO > = 40 |
| Age 0-64 | $100 | $150 |
|
Age 65+ |
$120 | $180 |
New graduate in a patient enrolment model: fee code TBD
| Newly enrolled patient | RIO < 40 | RIO > = 40 |
| Age 0-64 | $150 | $225 |
|
Age 65+ |
$180 | $270 |
Yes. Specifically, you will be able to claim the Patient Attachment Bonus, the Health Care Connect – Complex/Vulnerable and Mother/Newborn bonuses for new patients who were enrolled on or after July 1, 2025. The parties will notify members how this can be done once implementation of the codes occur as we recognize stale dating rules have passed.
This bonus is an upgrade from $350 to $500. It is for enrolling unattached patients who:
- Are referred from the Health Care Connect waitlist and are identified by Health Care Connect as complex and/or vulnerable
- Were not identified as complex and/or vulnerable by HCC, but which you later determine are complex and/or vulnerable
This bonus is available for enrolling both an unattached mother and newborn within two weeks of birth, or an unattached woman after 30 weeks of pregnancy. There is an additional bonus for enrolling each additional newborn attached after delivery in the case of multiple births (e.g. twins, triplets, etc.).
Only one attachment code can be billed per patient. If two are submitted for the same patient (e.g. the new patient attachment code and an HCC attachment code), the ministry will pay the higher of the two.
The only exception to this is mother newborn and multiple newborn, which can be billed together when applicable.
You can use the OMA RIO lookup tool to determine your office’s RIO score.
New graduates are defined as:
- Physicians who join a PEM within three years of completing a family medicine residency
- Physicians who join a PEM within three years of completing family medicine postgraduate training for International Medical Graduates and receiving an independent practice licence; note that Practice Ready Ontario physicians have three years from when they are issued a CPSO number
New graduate eligibility begins when you join the PEM and continues for 12 months.
An established doctor is a physician who completed family medicine residency more than three years ago.
No, only those physicians that have completed family medicine postgraduate training and received a license to practice within the previous 3 years are considered a new graduate. In this case, you would be eligible for the existing doctor rate.
Yes, provided all criteria is met, physicians on Income Stabilization are eligible for all categories of patient attachment bonuses.
The new Patient Attachment Bonus, the new Health Care Connect Complex/Vulnerable and Mother/Newborn codes are not yet available. The other bonuses are available and should be billed as you would other codes.
For the Patient Attachment Bonus, once the fee codes become available, you will be able to claim them retroactively. You will need to back-date the service date to the first billable service in the usual family practice setting, either on or after the date of enrolment.
Once the fee codes are available, the Patient Attachment Bonus for prospectively enrolled patients can only be paid if the patient is enrolled to the physician (e.g. using a Q200). The bonus can only be billed for a newly enrolled patient at the time of the first billable service. The first billable service does not include services provided outside of the usual family medicine clinical practice setting prior to enrolment. The service may be provided on the same day as enrolment or at the next visit after enrolment.
The current Health Care Connect Complex/Vulnerable patient bonus can be billed now using fee code Q053A. The top up under the new code will be paid retroactively, once it is available. You will not need to resubmit the code.
Assuming each patient meets the requirements of the appropriate bonus fee code, there is no limit on how many patients you can bill for. Note that only one patient attachment bonus code can be billed per patient per group.
The new patient attachment bonus codes are not yet available for billing. We are currently working through the implementation details with the Ministry of Health.
Provided that your patients are eligible and you meet all billing requirements, once the patient attachment bonus codes are available, claims can be submitted retroactively to July 1, 2025.
Only one attachment code can be billed per patient. If two codes are submitted for the same patient (e.g. the new attachment code and an HCC attachment code) the ministry will pay the higher of the two (again, assuming criteria are met).
The only exception to this is mother newborn and multiple newborn, which can be billed together when applicable.
No. If you are taking over a physician’s roster there is no break in attachment, the patients are not "unattached," which is the purpose of this bonus.
No. The patient attachment bonus only applies to eligible patients rostered from July 1, 2025 forward. However, the attachment bonuses under the other categories (e.g. FIT Positive, Acute inpatient stay, Health Care Connect Complex/Vulnerable) were available prior to July 1, 2025.
Yes, as long as the physician who passed away was not a member of the enrolling group. One of the criteria on the form is ‘The patient’s physician is no longer available due to illness/death/retirement.’ As such if this clause is met you can bill the bonus for this patient.
Yes, one of the criteria on the form is ‘The patient has moved to another community’, as such you can bill the bonus for this patient.
No. If the patient has ever been enrolled to you – in any group – you cannot claim the patient attachment bonus for them.
Yes. As long as they meet the eligibility criteria:
- They meet the definition of “New Patient”
- They, or their substitute decision makers, complete the requisite forms
- You’ve submitted the relevant enrolment code (Q202)
A patient attachment bonus is only eligible for newborns in the following cases:
- When both a newborn and unattached mother are enrolled together: Mother newborn new patient fee ($350, fee code TBD)
- For each additional newborn attached in the case of multiple births: Multiple/newborn fee ($150, fee code TBD)
If any of your existing patients, enrolled or not, have a new baby that baby would not be considered a new patient for the purposes of this fee.
No. If the fee code is billed by any member of the group for a specific patient, it cannot be billed again for the same patient within the same group.
Previous fee-for-service would not count and you may be eligible. However, keep in mind that the patient must meet the criteria in the New Patient Declaration form to be eligible for payment.
To enrol a patient, have the patient complete, sign and date the Patient Enrolment and Consent to Release Personal Health Information form. Then you should submit the appropriate enrolment fee code (e.g. Q200A). Note the date on the enrolment form must have the same date as the Q200 submission.
You can ask the patient and rely on their response. Currently, there is no central place where you can check if the patient is enrolled anywhere else.
There are two patient declaration forms. Most new patient attachment bonuses are tied to the New Patient Declaration Form, which is available online.
The New Patient Declaration form is not needed for normal enrolment; it is only needed for claiming the patient attachment bonus.
The declaration enables you and the patient to confirm that the patient is indeed unattached (i.e. who is not currently under the care of another Ontario family physician). It also confirms that you accept the patient into your practice.
For prospectively enrolled patients:
You can either email the New Patient Declaration form to the patient and have them sign it, or you can have them sign and date the form on their first visit.
For retroactively enrolled patients (back to July 1, 2025):
Stand by for instructions from the ministry.
Yes, the New Patient Declaration form can be signed electronically by the patient and sent back to physician, or the patient can sign in-person.
Copies of the completed forms must be kept in the patient’s chart for audit purposes. They do not need to be submitted to the Ministry. Electronic copies in the chart are sufficient; paper copies do not need to be kept.
The ministry will periodically review claims for the new patient attachment bonus. The review may include an audit of signed and dated New Patient Declaration forms, or contact with either the physician or patient, to verify the accuracy of the claims for the new patient attachment bonus.
Yes. You must submit the appropriate enrolment code (e.g. Q200A) for all enrolled patients. These zero-value fee codes tell the ministry which patients are rostered to you. They must be submitted in order to be eligible for the new Patient Attachment Bonus.
Yes, comprehensive virtual care will count as a first billable service.
If the physician chooses to de-enrol a new patient within 12 months of formal enrolment, the fee for the patient attachment bonus paid to the group will be recovered.
Co-location
They apply to existing FHO groups if they want to add a new site. They also apply to all new FHOs.
The minimum FHO size has not changed; it is six physicians.
Existing FHOs may continue to operate in accordance with their previous group size, including any approved exemption, until the exemption expires (if applicable) or their group size increases to six physicians, whichever comes first.
New FHOs must have a minimum of six physicians, unless the FHO has obtained the approval of the MOH in writing to have fewer than six physicians (see sections 2.3 and 2.4 of the updated FHO contract).
If all physicians in a FHO cannot be in the same location, there should be no less than two physicians in each location.
- Where the primary site has a RIO score of zero, all FHO locations should be within a five km radius of one another
- Where the primary site has a RIO score of one to five, all FHO locations should be within a 10 km radius of one another
- Where the primary site has a RIO score greater than five, all FHO locations should be within a 30 km radius of one another
No, as this is not a "new" site, the physician can continue to work here as a solo site.
The ministry would use the FHO’s primary/base location (i.e. the lead physician’s address) for the RIO score. For example, if the FHO’s base location has a RIO score of 25, additional sites for the group would need to be within a 30 km radius of the primary location.
Group Management Leadership Payment
Both the GMLP and the new enhanced GMLP are administrative payments to the FHO group that compensate for leadership of the FHO.
The GMLP existed before April 1, 2026. It pays $1 per rostered patient per year, prorated daily up to a maximum of $25,000 per year.
The enhanced GMLP is effective as of April 1, 2026. It pays an additional $4 per rostered patient per year, prorated daily up to a maximum of $100,000 per year.
The current GMLP and the new enhanced GMLP combined will pay each FHO a minimum of $25,000 per year.
You do not need to apply for it. FHOs are automatically entitled to the enhanced GMLP under the 2026 FHO contract (see section 11.1(b) of Appendix “I” to the contract).
The current GMLP is $1 per rostered patient, up to a maximum of $25,000 per year. In addition, an enhanced GMLP came into effect on April 1, 2026, which is a further $4 per rostered patient, up to a maximum of $100,000. This means that in total, physicians will get $5 per rostered patient, up to a maximum of $125,000 per year.
The GMLP is intended to compensate FHO Leads for providing leadership to ensure compliance with the FHO contract in a general sense, including appropriate after-hours availability and coverage. It can be used for a variety of activities, at the group’s discretion.
You are not required to document activities related to the GMLP.
The GMLP is paid to the FHO, not the FHO physicians or FHO contracted physicians, as it is provided in return for the leadership of the FHO specifically. It is up to the FHO’s discretion how to allocate the GMLP.
You can push back on this request. The GMLP is provided in return for clinical leadership activities, not administrative or managerial functions.
The GMLP is paid monthly and prorated as appropriate. The enhanced GMLP will ultimately be paid monthly starting April 1, 2027; however, for the first year, the payments will be quarterly.
The Ministry of Health does not deduct HST from the GMLP or enhanced GMLP payments, as they are payments “payable or reimbursed by the government of a province, under a plan established under an act of the legislature of the province to provide for health-care services for all insured persons of the province.”
The GMLP and enhanced GMLP payments will show up in the form of a deposit into the FHO group account. Section 3.1 of Appendix “I” to the 2026 FHO contract requires that the GMLP and enhanced GMLP payments will be issued to the FHO, not individual FHO physicians or FHO contracted physicians.
No, the enhanced GMLP is only available to FHOs.
No. The OPA payment is not going away. See sections 3.1, 11.2, and 11.3 of Appendix “I” to the updated FHO contract, which set out the entitlement to and eligibility for the OPA payment.