
Improving your Continuity of Care measure
As the new FHO+ model is implemented, FHO physicians will start to see data about their continuity of care levels. Monthly continuity of care reports are now being sent by email to your FHO Leads for distribution to the group.
As these reports come to you, you may have questions about what’s next. Here’s some information to keep in mind.
The monthly report provides timely feedback but isn’t the full picture
As a reminder, the monthly report does not represent complete data. It only represents data for claims that were submitted in the previous month. For example, your May Continuity of Care report includes data for claims submitted in April only. Because physicians have 90 days from the service date to submit claims, the monthly reports won’t necessarily represent the full picture.
Secondly, it is continuity of care over the quarter that is evaluated. The monthly measure is not what triggers an adjustment. Even if you are below 75 per cent for two months, it is still possible for your quarter’s overall measure to be above 75 per cent.
OMA template letter for patients
A template letter for patients encouraging them to seek care within your FHO group.
Remember what triggers a financial adjustment
Monthly continuity of care rates do not trigger a capitation adjustment.
The trigger for a capitation payment adjustment is that two related measurement quarters are both below 75 per cent. The related measurement quarters are three quarters apart, Qx + 3 (for example, Q1 and Q4).
It is possible to be below 75 per cent for a quarter and face no capitation adjustment, ever. It is even possible to be below 75 per cent for multiple quarters in a year and not face a capitation adjustment. It’s all about the timing.
Learn more about what triggers a capitation adjustment and access a calculator to play with different quarterly percentages to see how and when they affect capitation payments.
Steps you can take now
Because your monthly continuity of care report doesn't represent the full picture, it may be helpful to avoid making major changes based on this interim data alone. You may want to wait and see what happens for your first full quarter (April-June).
That said, if you want to be proactive, here are some steps you can take now.
1. Confirm your understanding of how continuity of care is calculated
Continuity of care is evaluated on a quarterly basis using this calculation: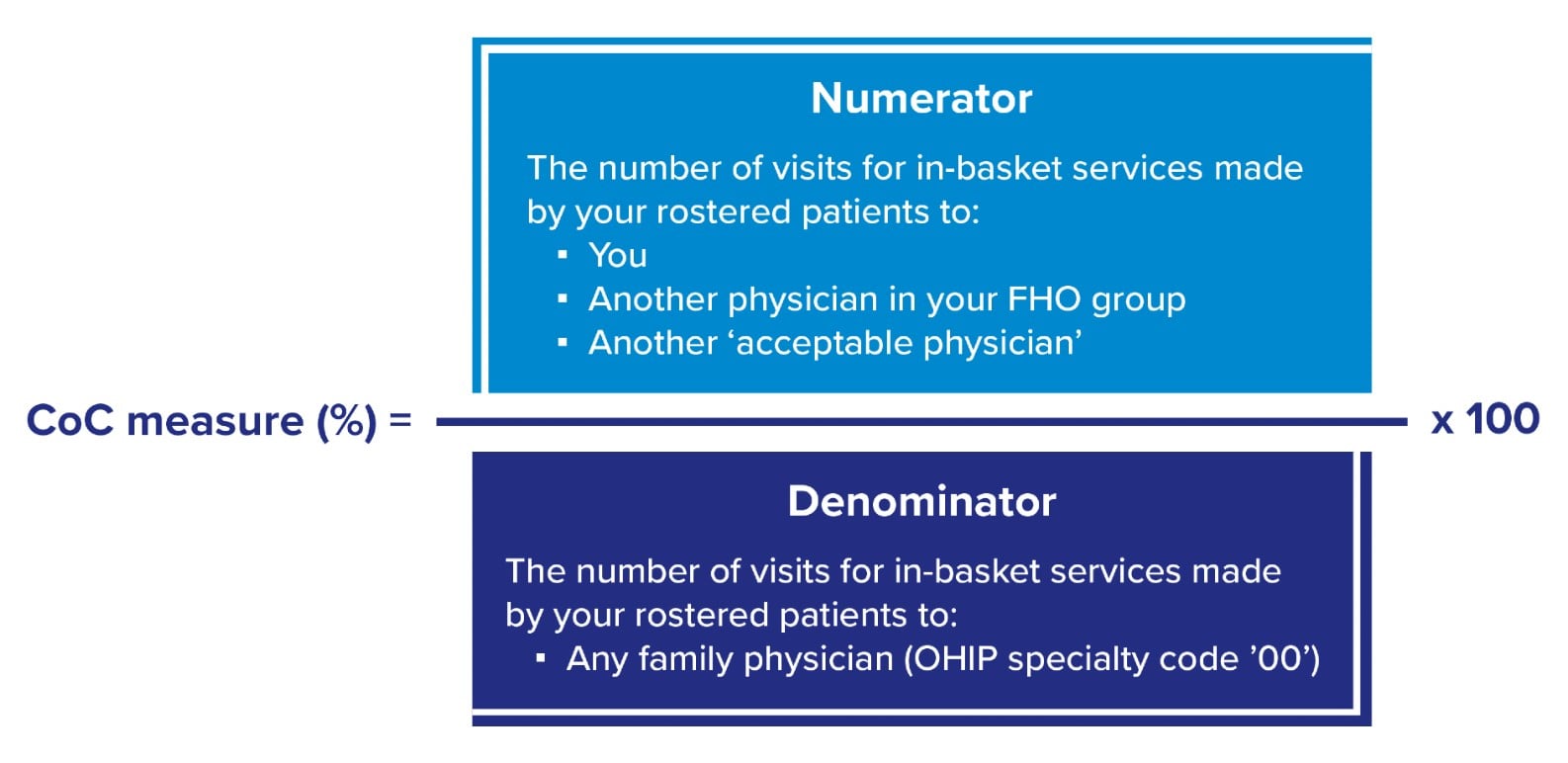
New with FHO+ is that visits by your rostered patients to an "Acceptable Physician" for in-basket services now count in your favour.
Acceptable Physicians include:
- Designated GP focused practice physicians (including GP psychotherapy) for in-basket visits using fee or diagnostic codes identified for their area of practice
- HIV or Care of Elderly (COE) physicians billing in-basket fee codes
- Physicians providing visits for in-basket services that take place in an ED or elsewhere in a hospital as identified by a master hospital number, including special visits to an ED using codes K990-K999, H980-H981, H984-H989
- Physicians billing ocular-visual fee codes A110A and A112A
Refresh yourself on the current list of in-basket fee codes.
2. Review your outside use report
In addition to the monthly continuity of care report, you will continue to receive your outside use report.
Here is a comparison of what’s changed with FHO+ when it comes to the impact of patient visits to physicians outside of your practice:
Here is a comparison of what’s changed with FHO+ when it comes to the impact of patient visits to family physicians outside of your practice:
| FHNs and negation
Note: this is what is reflected on the outside use report |
FHO+ and Continuity of Care | |
|---|---|---|
| Counts towards you |
In-basket services provided by:
|
In-basket services provided by:
|
| Counts against you |
In-basket services provided by:
|
In-basket services provided by:
|
| Financial impact | Dollar-for-dollar reduction each time a rostered patient seeks care outside of the group for in-basket services | No impact unless continuity of care measure for your roster falls below the continuity threshold of 75 per cent in two related measurement quarters |
3. Familiarize yourself with the GP Focused Practice physicians in your area
You can access a list of all GP focused practice physicians.
For patients seeing a specialty-focused GP, encourage them to see a one with a formal Focused Practice designation and offer to make the connection for them.
4. Communicate with your patients
It’s fair to communicate with your patients to let them know what services your FHO group offers and to help them understand what continuity of care is and how it benefits them.
Consider an email blast or printed mailout to let them know. You can include content like:
- Reminder of your After Hours availability and how to book
- Availability of virtual care options and what kinds of issues they are suitable for, if applicable in your practice
- Information about what GP Focused Practice physicians are
- The benefits of continuity of care
Access an OMA template letter for patients to encourage them to seek care within your FHO group.